


The famous musician Seal is known for his numerous international hits, and for living with an autoimmune disease: the scars on his face are the result of discoid lupus erythematosus. Picture: C. Grube for Access2music.de, wikimedia
Systemic lupus erythematosus (SLE) is a chronic inflammatory disease with manifold manifestations. SLE belongs to the family of autoimmune disorders, diseases that occur, when a mislead immune system attacks the body’s own structures. SLE can affect almost any organ system, thus its presentation and course are highly variable, and diagnosis and therapy may be challenging.
With the intention to classify SLE patients for research and surveillance studies and to support clinicians in confirming a diagnosis, a set of clinical and laboratory classification criteria has been developed and released by the American College of Rheumatology (ACR). The first classification criteria for SLE were originally published in 1971 [1,2]. They have been updated 1982 [3] and 1997 [4] to incorporate new immunologic knowledge and improve patient classification. In contrast to the 1987 criteria, the 1997 criteria have not been validated.
The most recent addendum to the classification criteria for SLE dates from 2012, when the Systemic Lupus International Collaborating Clinics (SLICC) group published a revision and validation of the ACR criteria [5].
The SLICC group is an international group of investigators dedicated to clinical research on SLE. With the intention to improve the clinical relevance of the ACR criteria, they incorporated recent findings on the immunology of SLE and addressed several problems that were attributed to the 1982/1997 criteria, and they performed the so far missing validation. According to the SLICC experts, validation of the new criteria resulted in high sensitivity and specificity, resulting in fewer misqualifications compared to the 1982/1997 criteria.
In conclusion, the SLICC group identified eleven clinical and six immunologic criteria. Because SLE is an antibody-driven clinical disease, neither clinical criteria nor positive serological test results alone should be considered as diagnostic of SLE.
According to the SLICC rule a patient has to fulfill at least four criteria, including one clinical and one immunologic criterion. In addition, the scientists defined a new “Stand alone” clinical criterion: biopsy-proven lupus nephritis. Consequently, lupus nephritis together with the presence of antinuclear or anti-double-stranded DNA antibodies is sufficient to definitely classify a patient as having SLE.
How the experts proceeded — Step one: identifying appropriate criteria
The members of the SLICC consortium started with the derivation of an initial set of defined variables, which they extracted from the medical reports and laboratory data of patients presenting in the participating medical centers.
Each center provided data on a specified number of patients with a definite diagnosis of SLE, and an equal number of patients with the diagnosis of another rheumatologic disease, e.g. rheumatoid arthritis, myositis, chronic cutaneous lupus erythematosus, undifferentiated connective tissue disease, vasculitis, Sjögren’s syndrome, antiphospholipid syndrome or scleroderma. From this data pool containing the records of 716 patients (293 SLE, 423 other rheumatic diseases), the SLICC scientists derived a set of preliminary criteria for classifying SLE. The selection resulted from a statistical analysis of the data refined by a consensus decision of the paricipatin clinical resaechers. Initially, they found 18 criteria, divided into the categories clinical or immunological. After discussion of misclassified cases, some definitions were refined or combined, resulting in the final list of eleven clinical and six immunological criteria.
Clinical Criteria
- Acute cutaneous lupus
- Chronic cutaneous lupus
- Oral or nasopharyngeal ulcerations
- Nonscarring alopecia
- Synovitis involving two or more joints
- Serositis
- Renal disorder
- Neurologic disorder
- Hemolytic anemia
- Leukopenia or lymphopenia
- Thrombocytopenia
Immunologic criteria
- ANA level above laboratory reference range
- Anti-dsDNA antibody level above laboratory reference range
- Anti-Sm presence
- Antiphospholipid antibody positive, by any of the following:
-medium or high titer anti-cardiolipin
-positive test for anti-beta-2-glycoprotein- Low complement
- Direct Coombs’ test in the absence of hemolytic anemia
Step two: Validation of the new criteria
In an intensive process of evaluation, the SLICC experts validated the preliminary criteria based on a second independent data set. In order to test their performance, the SLICC experts applied the provisional criteria to 690 additional patients with a diagnosis of SLE (337 patients) or another rheumatologic disease (353 patients).
A comparison of the proposed SLICC criteria and the current 1997 ACR criteria in the validation cohort showed a better performance of the SLICC rule with higher sensitivity and fewer misclassifications of patients.
According to the SLICC authors, the new clinical criteria improve the 1997 ACR criteria in several ways. The dermatological conditions malar rash and photosensitivity are no longer separate items; in fact, they are largely overlapping. One criterion for acute cutaneous lupus covers both, acute and subacute forms. A separate criterion now includes discoid rash and the many different types of chronic cutaneous lupus, which are not represented in the current ACR criteria. Alopecia is again included, as it was in the first criteria set form 1971.
Major changes apply to the arthritis criterion, taking into account that lupus related arthritis may also be erosive, the requirement for non-erosive arthritis has been removed. The arthritis criterion now comprises synovitis, swelling, tenderness and morning stiffness. Important caveat, especially when lupus arthritis is concerned, but also with respect to any other clinical criterion: the clinician must be able to determine that the symptoms are attributable to SLE and not to any other disease.
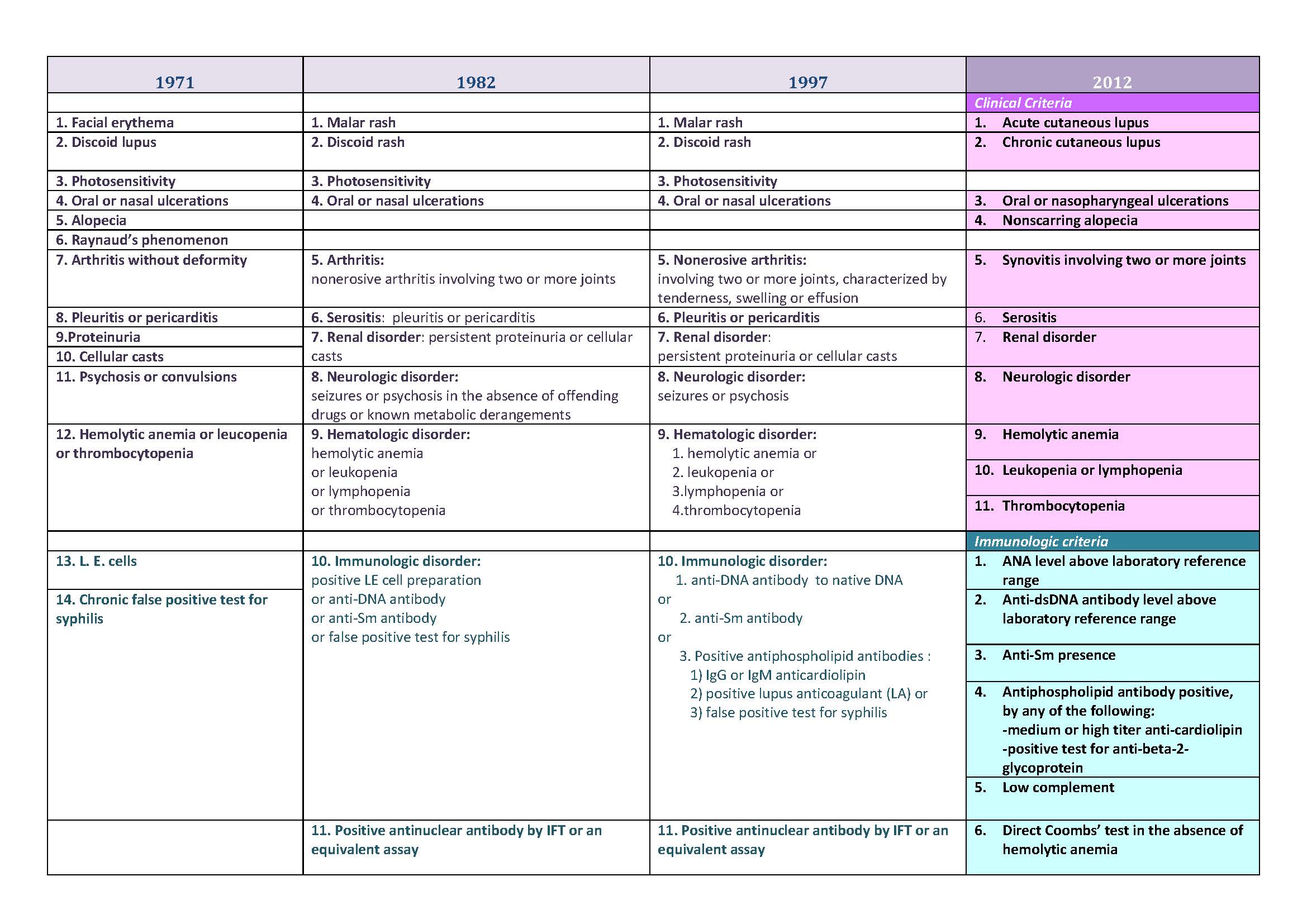
A detailed comparison of the classification criteria from 1971, 1982, 1997 and 2012 is depicted in the table below.
The revised immunologic criteria reflect new insights into SLE serology and take into account the wider use of ELISA assays. The established ANA criterion remains unchanged. Anti-dsDNA antibodies, anti-SM antibodies and antiphospholipid antibodies are no longer a combination item, they were separated into single parameters and each may contribute independently to classification. Antibodies to anti-beta-2-glycoprotein now complement the panel of antiphospholipid antibodies. All individual isotypes, IgG, IgM and IgA for anti-beta-2-glycoprotein and anti-cardiolipin have been included. This reflects recent findings that IgA isotypes are strongly associated with clinical manifestations in SLE.[5]
Two years after their publication the SLICC criteria still have the character of a proposal or recommendation. The ACR website features the 1997 Update of the 1982 criteria, which perform well compared with the “gold standard” of diagnosis by a skilled physician. However, they do not include the updated and more extended variables defined in the SLICC criteria. The new SLICC criteria provide a comprehensive alternative for use in clinical care and research, offering a more differentiated picture of the autoimmune processes in lupus patients .
Both the ACR revised criteria and the validated SLICC criteria are designed for classification of patients for clinical studies and have not been tested for purposes of diagnosis.The SLICC criteria are more consistent with advancing concepts of SLE, and they will exert substantial impact on clinical practice. Real diagnostic criteria for nonspecialists are still an unmet need in SLE and the SLICC classification criteria contribute to partially fill in this gap.
References
1. Cohen, A. S. et al., Bulletin on Rheumatic Diseases, 1971, 21:643.
2. Davis,P., Atkins,B., Josse,R.G., and Hughes,G.R., Criteria for classification of S.L.E. Br Med J 1973. 3: 88.
-> Link to full text article
3. Tan,E.M., Cohen,A.S., Fries,J.F., Masi,A.T., McShane,D.J., Rothfield,N.F., Schaller,J.G., Talal,N., and Winchester,R.J., The 1982 revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1982. 25: 1271.
-> link to abstract in PubMed
-> Table: The 1982 updated ACR criteria
4. Hochberg,M.C., Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum 1997. 40: 1725.
-> Link to abstract in PubMed
5. Petri,M., Orbai,A.M., Alarcon,G.S., Gordon,C., Merrill,J.T., Fortin,P.R., Bruce,I.N., Isenberg,D., Wallace,D.J., Nived,O., Sturfelt,G., Ramsey-Goldman,R., Bae,S.C., Hanly,J.G., Sanchez-Guerrero,J., Clarke,A., Aranow,C., Manzi,S., Urowitz,M., Gladman,D., Kalunian,K., Costner,M., Werth,V.P., Zoma,A., Bernatsky,S., Ruiz-Irastorza,G., Khamashta,M.A., Jacobsen,S., Buyon,J.P., Maddison,P., Dooley,M.A., van Vollenhoven,R.F., Ginzler,E., Stoll,T., Peschken,C., Jorizzo,J.L., Callen,J.P., Lim,S.S., Fessler,B.J., Inanc,M., Kamen,D.L., Rahman,A., Steinsson,K., Franks,A.G., Jr., Sigler,L., Hameed,S., Fang,H., Pham,N., Brey,R., Weisman,M.H., McGwin,G., Jr., and Magder,L.S., Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum 2012. 64: 2677.
-> Link to Full text article
6. Mehrani,T. and Petri,M., Association of IgA Anti-beta2 glycoprotein I with clinical and laboratory manifestations of systemic lupus erythematosus. J Rheumatol 2011. 38: 64.
-> Article Abstract in PubMed
[/pc-pvt-content]